Cocaine: more deadly in the male
The figures we reported yesterday in Part 2 of our series on drug-related deaths show that cocaine has been implicated in five times as many deaths among men as among women.
Can this be because the ratio of cocaine use among men and women is equally extreme? Or is there some other explanation? For answers, we turn to successive sweeps of the British Crime Survey (BCS) in the 21st century. For our definitions, see earlier articles in the series, or the footnote to this article.
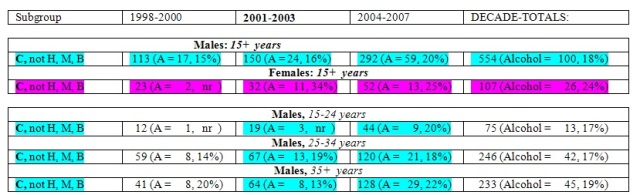
Deaths caused by cocaine increased from 136 in 1999-2000 (or 45 per annum) to 182 in 2001-2003 (61 per annum) and then by 40 per cent to 344 in the four years of 2004-2007 (86 per annum). See Table 1, below:
The data from the British Crime Survey (Table 2) shows that cocaine-use in the past year was reported by 6.8 per cent (95 per cent CI: 6.3 to 7.4 per cent) of 16-24 year old male respondents in the three sweeps of the BCS (2003/04, 2004/05 and 2006/07) and by 3.9 per cent of similarly aged female respondents (CI: 3.5 to 4.3 per cent).
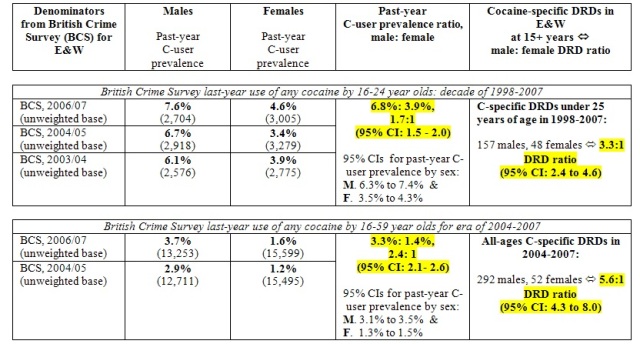
From these, we can work out the ratio between males and female users as 1.7: 1 (CI: 1.5 to 2.0). By contrast, for the decade of 1998-2007, the ratios of deaths specifically related to cocaine use was 157: 48 or 3.3:1 (CI: 2.4 to 4.6) which is about twice the sex ratio.
Table 2 also shows the corresponding all-ages data for the recent era of 2004-2007 (during which most C-specific deaths were observed). Notice that 3.3 per cent of adult male respondents to BCS in 2004/05 and 2006/07 reported past-year use of cocaine but only 1.4 per cent of female respondents did so, a male: female ratio of 2.4: 1 (CI: 2.1- 2.6) while the male: female ratio of cocaine-specific deaths in 2004-2007 was 292: 52, or 5.6:1 ( CI: 4.3 to 8.0).
So whether we focus on 16-24 year olds, or 16-59 year olds, death rates are about 2.4 times as high in men as they are in women.
Precisely why remains a mystery. Age is not a confounder because the same risk multiplier applies at 16-24 years as at all-ages. Nor does alcohol provide a ready explanation, as its co-presence is noted more often at C-specific deaths for females (24 per cent: 26/107) than for males (18 per cent: 100/554). Intensity of cocaine-use could be different between the sexes (but was not reported for male versus female users by BCS); or, improbably, toxicology may be different, or reported differently, for male deaths than for female ones.
Whatever the reason, males need to be warned that they run twice the risk of dying as a result of their cocaine use than do their female counterparts. Tomorrow, we reveal just how sharply the risk of cocaine-related death increases with age.
Our definitions: Each of 15,795 DRDs was cross-classified by era of registration (1998-2000, 2001-2003, 2004-2007), sex, age-group at death (15-24, 25-34, 35+ years), presence/absence of heroin/morphine (hereafter, H), presence/absence of methadone (M), presence/absence of cocaine (C), presence/absence of benzodiazepines (B), and presence/absence of alcohol (A).
We define cause-specific DRDs as DRDs with “one specified illegal drug present and three other specified illegal drugs absent” such as “H, not (M, C, B)” [H-specific] or “M, not (H, C, B)” [M-specific] or “C, not (H, M, B)” [C-specific].
Conflicts of interest: SMB serves on, and was inaugural chair of, the Surveys, Design and Statistics Subcommittee (SDSSC) of Home Office’s Scientific Advisory Committee. In 2008, SDSSC reported on 21st Century Drugs and Statistical Science. Authors have research or clinical interests in the epidemiology and prevention of drugs-related deaths. SMB holds GSK shares and MRC-funding as part of the NIQUAD cluster on quantifying drugs harms.
