Heroin addiction: male risk higher than female
So far, from elementary evidence synthesis, we have discovered:
Cocaine-related drug-related death risk at least double that for Ecstasy: in 2004-2007, the risk across of dying as a result of cocaine was estimated at 22 per 100,000 people aged 16-59 who had used it in the past year but . . .
Cocaine-related death-rate increases sharply with age: in 2004-2007, the risk of dying as a cocaine user was estimated at 7 (95 per cent CI: 5.8 to 8.5) per 100,000 users, aged 16 to 24 but at 53 (CI: 47 to 59) per 100,000 of those aged over 35.
Increasing lethality of cocaine for older users in more recent years: the risk of death for older users was 37 (CI: 31 to 43) per 100,000 in 2001-2003 but 53 (CI: 47 to 59) per 100,000 in 2004-07. Why?
Male users run twice the risk of females: the risk multiplier in 2004-2007 was 2.4 (CI: 1.7 to 3.4).
Frankly, this intelligence needs to be communicated to users and their families as well as being understood by addiction scientists, drugs workers, GPs, policy-makers and also by Ministers.
Neither Ministers with responsibility for public health, home affairs or justice nor their policy advisors should contemplate changes to European drugs policies without having a sufficient understanding of how lethality differs between drugs, over time; and of how users’ sex and age-group may be stark risk-multipliers.
Simplistic messages won’t do. Let’s get serious: lethality differs between drugs, and for whom. The public, and users in particular, need a proper quantitative understanding of which drugs kill, and who is at greatest risk.
In the 21st century, the UK invested wisely in a suite of capture-recapture studies by which to estimate the number of problem drug users, who include injection drug users (IDUs).
Today, we exploit Bayesian capture-recapture estimates of the number of current IDUs (to nearest 100) for England which King, Hay, Hutchinson and Bird produced for a Home Office report on 21st Century Drugs and Statistical Science and which, here, we take as ‘representative’ for the era 2004-2007.
Male injectors’ have double the risk of heroin-specific death
Most, but not all, heroin-related deaths occur in injection drug users (IDUs). Heroin-specific DRDs accounted for 79 per cent of H-related DRDs (6,263/7,889) in England and Wales in the decade between 1998 and 2007. Here, we focus on H-specific DRDs, of which there were 2,400 in 2004-2007: 2,071 males and 329 females.
Is so extreme a male: female ratio as 6.3:1 for heroin-specific deaths in 2004-2007 matched by a correspondingly extreme sex ratio in current injection-drug users?
Table. Injecting drug user (IDU) denominators for Heroin-specific DRDs.
{Notice geographical mismatch between H-specific DRDs, which are for England and Wales, and IDU estimates, which are for England only (and so may under-estimate more geographically-appropriate IDU counts by 5% to 10%)}
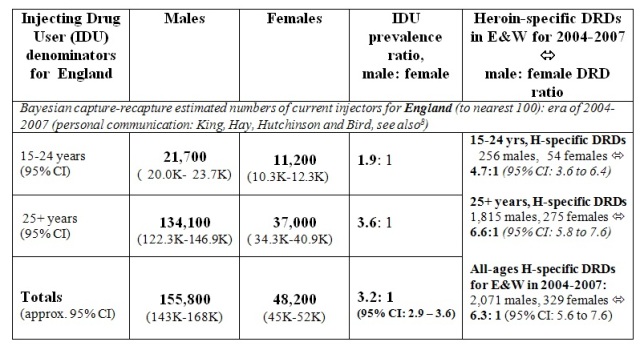
Current injectors are a relevant, but imperfect, denominator for H-specific DRDs as H-specific DRDs do not occur solely among IDUs. Derived by Bayesian capture-recapture analysis of English data from 2004/052, our Table shows then-current injectors (to the nearest 100) to have been estimated at 155,800 males and 48,200 females. A minority of current IDUs was 15-24 years old (around 33,000), and the male: female IDU ratio was more extreme among older injectors, being 3.6: 1 versus 1.9:1.
Male injectors outnumbered females by 3.2:1 (95% CI: 2.9 to 3.6) but the male: female ratio for H-specific DRDs was more extreme at 6.3:1, as we have seen.
Thus, taking IDU denominators into account, the relative risk of H-specific DRD appears to be nearly twice as high for male as for female IDUs with a risk multiplier of 2.0 (CI: 1.7 to 2.3). {By age, male IDUs’ relative disadvantage in terms of H-specific DRDs is conveyed by risk multipliers of 2.4 at 15-24 years versus 1.8 at 25+ years.}
Setting aside the geographical mismatch between our numerator (H-specific DRDs for E&W) and denominator (IDUs for England only), and remembering that not all H-specific DRDs occur to current IDUs, the per-annum H-specific DRD rates per 100,000 current injectors in 2004-2007 worked out roughly as follows (to nearest 10):
for male current IDUs : 290 ( CI, Poisson variation only: 260 to 330) at 15-24 years
and 340 (CI: 320 to 350) otherwise;
for female current IDUs: 120 (CI, Poisson variation only: 90 to 150) at 15-24 years
and 190 (CI: 160 to 210) otherwise.
Even the highest C-related DRD risk per 100,000 past-year cocaine-users, that for 35+ year olds, and of the order of 50 to 60, pales against the H-specific DRD rates per 100,000 current IDUs. Ecstasy-related DRD risk of 10 per 100,000 past-year Ecstasy-users is lower by a factor of 10 to 30.
Is males’ H-specific DRD risk mitigated by methadone? In Part 2 we remarked that, over the decade of 1998-2007, the male: female ratio for methadone-specific DRDs was 1,279: 333, or 3.8: 1, and so much lower than for H-specific DRDs.
For England only, the National Drug Treatment Agency was able to provide us with information by sex on the number of clients given opioid substitutes (mainly methadone) by specialist or GP prescribers in the each of the financial years 2005/06 to 2007/08. Totalled, these were 254,400 males (to nearest 100) and 102,200 females, which gave a male: female ratio of 2.5: 1 for those in receipt of mainly methadone substitutes.
In 2004-2007, the male: female ratio of M-specific DRDs was 461:145, or 3.2:1 (CI: 2.7 to 3.9) which makes for a risk multiplier of 1.3 (CI: 1.1 to 1.5) only.
A particular attribute of recruiting males into opioid substitution therapy may be to mitigate their heroin-vulnerability. For a wider account of the life-saving benefit of methadone substitution, see the analysis by Cornish et al. in last week’s BMJ.
Our definitions again: Each of 15,795 DRDs was cross-classified by era of registration (1998-2000, 2001-2003, 2004-2007), sex, age-group at death (15-24, 25-34, 35+ years), presence/absence of heroin/morphine (hereafter, H), presence/absence of methadone (M), presence/absence of cocaine (C), presence/absence of benzodiazepines (B), and presence/absence of alcohol (A).
We define cause-specific DRDs as DRDs with “one specified illegal drug present and three other specified illegal drugs absent” such as “H, not (M, C, B)” [H-specific] or “M, not (H, C, B)” [M-specific] or “C, not (H, M, B)” [C-specific].
Conflicts of interest: SMB serves on, and was inaugural chair of, the Surveys, Design and Statistics Subcommittee (SDSSC) of Home Office’s Scientific Advisory Committee. In 2008, SDSSC reported on 21st Century Drugs and Statistical Science. Authors have research or clinical interests in the epidemiology and prevention of drugs-related deaths. SMB holds GSK shares and MRC-funding as part of the NIQUAD cluster on quantifying drugs harms.
