Breast cancer: it's your fault
There’s nothing like a breast cancer story to get the media stirred up. And if you can tie it in with obesity and booze, stand back or you’ll be trampled in the rush.
Last week’s effort came from Cancer Research UK, which issued a press release headed “One woman in eight will get breast cancer”. It read: “The lifetime risk of getting breast cancer has risen from one woman in nine to one in eight” which sounded alarming enough to create a small stampede.
The item was high up in the BBC’s lunchtime bulletin on Friday – a notably uninformative report which gave viewers very little of the actual story but included, inevitably, a case history – and it also appeared in virtually every newspaper the same day: The Times, the Daily Express, The Press & Journal, the Evening Express, The Scotsman, The Guardian, The Sun, the Daily Mirror, the Daily Record, The Independent, Metro, The Herald, the Daily Mail, and probably some others. Trebles all round! (As Private Eye is wont to say.)
Some implied the death toll is rising (The Scotsman, above) . It isn’t. Others flatly blamed obesity, when the causes are complex. But nobody seems to have subjected the statistics to a very demanding scrutiny, and CRUK didn’t help by referencing the claim to an unpublished paper submitted by Professor Peter Sasieni to the British Journal of Cancer. Who cares? CRUK are a helpful and likeable bunch, so no medical correspondent is going to rain on their parade.
The claim isn’t wrong, but the implications are. In response to my request, CRUK responded swiftly with answers to a few questions.
There is a long-established method for estimating lifetime risk, which calculates the number of cases that would occur within each age band of a particular birth cohort. According to this method, the lifetime risk for women of being diagnosed with breast cancer has been one in eight since 2003. The table below comes from the CRUK Statistical Information Team.
But this method overestimates the risk, because it does not take account of the fact that women can be diagnosed with breast cancer more than once in their lifetimes. This adjustment is made in Professor Sasieni’s method (see first two columns) and produces a slightly lower risk.
These columns shows a risk increasing to reach 12.51 per cent in 2008. This equates to one in 7.99, and since CRUK always adjusts its figures upwards, it quotes that as one in eight. The figure for 2007, 12.29 per cent, equates as one in 8.14, which CRUK rounds up to one in nine.
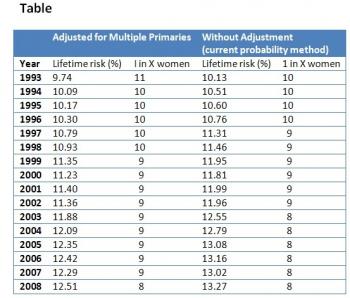
So the “big increase” in risk headlined by the papers from one in nine to one in eight is actually from one in 8.14 to one in 7.99. The lifetime risk has increased by 1.7 per cent, not (as the bare numbers imply) by more than 11 per cent.
Or, if you want to be picky, go back to 2006, when the risk equated to one in 8.05. That means it’s increased by 0.09 of a percentage point, or by 1.1 per cent, in two years.
If CRUK followed the normal convention for rounding numbers, the rate would have been expressed as one in eight ever since 2003, when it rose to one in 8.42. I can understand why they don’t – they don’t want to be accused of exaggerating – but isn’t the first sentence of the press release an equal exaggeration?
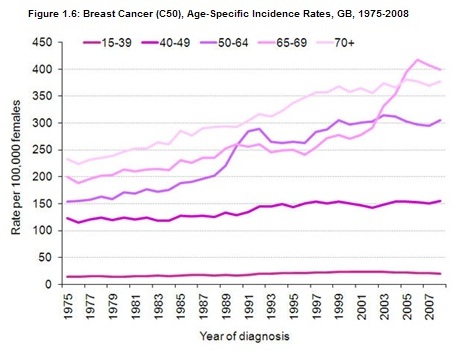
So what is the reason for the rise? Screening has a lot to do with it. Graphs of incidence for various age groups show a big surge after 1988 in the age group targeted (50-64) and another more recent surge in older women since 2004 as screening was extended to those 65-69. The rate in this age group has increased from around 300 per 100,000 women to over 400 in just a few years. (Source: CRUK)
This is also clear from the numbers published by the NHS Breast Screening Programme, which show a modest increase in the cancers detected in the 50-64 age group (10,033 to 10,990) between 2003-04 and 2007-08, but a bigger increase in the numbers detected in the 50-70 age group (12,387 to 15,567). It is clear that most of this rise is being driven by those between 65 and 70.
In rough terms, it looks as though screening has accounted for around 5,000 diagnoses in women aged 65-70 in the past five years, around 2.0 per cent of total diagnoses in that time. Some of these would have been detected without screening as they became apparent, but some would not. CRUK acknowledged (to me) that a proportion of the increased incidence is due to screening, but does not attempt to quantify it - nor was it mentioned in the press release.
It cites drinking, obesity, diet and the use of HRT as other risk factors. While there is evidence for all of these, the headlines exaggerated the real change that has taken place, ignored the effects of screening and left women with the disquieting message that it’s all their fault. See Metro's headline below:

Comment
Catherine Thomson, Head of Statistical Information at CRUK, has submitted the following comment, which the spam filter has for some reason rejected. In order to post it as quickly as possible, I am adding it to the body of the article rather than trying to bypass the filter. NH
"We do not believe that the first sentence of our press release is an exaggeration because we did not claim that the change happened suddenly between 2007 and 2008. Instead the press release relays an important message to the public in a simple way - namely that over the last decade the lifetime risk figure for breast cancer has risen to 1 in 8 from 1 in 9.
"Prior to our release last week Cancer Research UK, along with other charities and researchers, had been using data for 2001-2005 combined (the latest data we had available) which showed the risk was 1 in 9 (1 in 8.55, to be precise), obtained using an earlier version of the method we developed with Peter Sasieni. The figure of 1 in 8 that we published last week was based solely on 2008 data.
"In response to a request from Nigel Hawkes we provided him with an annual breakdown. These annual figures had not previously been calculated until the most recent data were available.
"If you look at these annual figures the change in risk from 2007 to 2008 is very small – but it reflects a gradual increase over the decade equating to a relative increase of over 10% in 10 years (from 1 in 8.81 to 1 in 7.99). Such a large increase in incidence risk for the most common cancer is newsworthy and it is important that this message is known.
"Obviously, there was not a step change in risk straight from 1 in 9 to 1 in 8 last week but in terms of a simple message being relayed to the public it helps to use whole numbers – since the general reader is less likely to understand fully such complex data than the readers of Straight Statistics.
"Many factors affect the risk of breast cancer and it is difficult to quantify exactly how much each of these has contributed to the rise in lifetime risk in the absence of detailed research. The press release referred to some established breast cancer risk factors, and suggested things women can do to help reduce their risk of breast cancer.
"We considered different factors in more detail In our blog post. These included screening, lifestyle factors, having children later, HRT and more.
"In summary, we did not over-estimate or exaggerate the claim. It was important to publicise widely the change in the message to ensure that both the public and those working in the cancer sector are aware of the true lifetime risk of breast cancer, and that using 1 in 9 is no longer correct."

Lee Hulbert-Williams (not verified) wrote,
Mon, 07/02/2011 - 19:35
Of course, it wouldn't be completely silly to just give figures to a greater number of decimals, or use x-in-a-hundred type expressions instead. Accuracy doesn't have to be confusing.
Great post by the way
Sumit Rahman (not verified) wrote,
Tue, 08/02/2011 - 09:26
1 in 8.14 to 1 in 7.99!! Well done for hunting this down!
Dr. Paul Foster (not verified) wrote,
Wed, 09/02/2011 - 14:49
An excellent piece of writing. Well done on tracking all this down.
Evan Harris (not verified) wrote,
Thu, 10/02/2011 - 08:44
This was an excellent article and - after I publicised it on twitter, asking if CRUK would respond - a prompt and helpful reply from CRUK which Nigel wisely has included in the text.
There are a number of issues that are of interest still:
1) It seems that this is the press release is here
http://info.cancerresearchuk.org/news/archive/pressrelease/2011-02-04-on...
It is a pity that neither Straight Statistics (nor CRUK) provide a link to it so that readers can see whether the first sentence was misleading in context. It seems to me that it does NOT make the claim that the increased risk is a year on year change, and that Ms Thomson's points in this respect are reasonable.
Evan Harris (not verified) wrote,
Thu, 10/02/2011 - 08:45
2) Why does CRUK press release data from an unpublished paper?
This is poor practice in my opinion since it prevents readers and interested parties from looking at peer reviewed detail or indeed any of the content of the paper other than that which CRUK choose to provide in their press release (or on their website at the time of the release, the embargo or subsequently).
The press release gives the figures and does not state their (unpublished source). The second of two references gives a link to the CRUK statistics page http://info.cancerresearchuk.org/cancerstats/types/breast/incidence/#Lif...
This in turn under the paragraph on Lifetime Risk says
"Breast cancer is by far the commonest cancer in women in the UK accounting for 31% of all cases in women. The next most common cancer in women is lung cancer, with 17,960 cases (12% of total) in 2008. So nearly a third of all new cancers in women are breast cancers. It has been estimated that the lifetime risk of developing breast cancer is 1 in 1,014 for men and 1 in 8 for women in the UK. [Ref 5]”
And Ref 5 merely says..
Sasieni PD, Shelton J, Ormiston-Smith NJ, Thomson CS, Silcocks PB. What is the lifetime risk of developing cancer?: The effect of adjusting for multiple primaries. [submitted] 2011
"Submitted" may mean not yet accepted for publication (as it may have said in press and given a journal if that were the case but I am not certain of the conventions here] and that means that it may not have been have been peer-reviewed, which in turn means that when published the claims may be different of hedged.
Evan Harris (not verified) wrote,
Thu, 10/02/2011 - 17:15
I have a point 3 that this site will not let me post! It crashes when I try. Grr!
Evan Harris (not verified) wrote,
Thu, 10/02/2011 - 17:16
3) It also seems that the important thing to do is to establish clearly whether there is any statistically significant increased risk of developing breast cancer once increased screening (detection) of breast cancer is accounted for. This is because the press release and media coverage focuses on increasing risk factors in recent years (eg delayed families, HRT use) and this would be misleading if the rise was due to increased screening rather than increased risk. As a corollary it would be absurd to have a situation where - by screening all 80-90 year olds for cancer - a large number of cancers were found which were not going to affect mortality (or even morbidity) if undiagnosed, and that this was translated into an increased risk of cancer and related to lifestyle risk factors for all women.
It may be that by re-analysing the figures without the 65-69 cohort (which had screening introduced in 2004 and has seen a large rise in incidence) there is no statistically significant overall increase in 0-64 risk - at least since routine screening for 50-64 year olds was introduced. This may or may not be the case but the press release does not deal with this at all and we cant see the paper (because it's unpublished) to see how this is tackled.
Evan Harris (not verified) wrote,
Thu, 10/02/2011 - 17:17
As I say above, the press release of 4th February links as the 2nd of its two references to this page on the CRUK website (updated 3rd February it says)
http://info.cancerresearchuk.org/cancerstats/types/breast/incidence/#Lif...
It says "The recent steep rise in rates for women aged 65-69 is almost certainly caused by the introduction of national breast cancer screening for this age-group (Figure 1.7 Refs 27, 38)" The refs are to the source of figure 1.6 (which is the one used by Straight Statistics above) not to the underpinning of the statement about increased incidence.
Nigel Hawkes (not verified) wrote,
Thu, 10/02/2011 - 17:36
In response to Evan and to CRUK, it is true that the press release does not imply that the change took place in a single year.
But the table CRUK sent me, and which I included in the artiicle, does imply that. There is an abrupt shift between 2007 and 2008 from one in nine to one in eight. This is, as I explained, an artefact of the way CRUK rounds up the figures.
Evan's point about whether cases ascertained by screening older women can account for the recent rise is a good one. I attempted to explore that but didn't get very far. The problem is that as screening is gradually extended both to younger and older women this particular issue will continue to muddy the waters.
Catherine Thomson (not verified) wrote,
Fri, 11/02/2011 - 17:05
We would like to clarify that Cancer Research UK did not publicise data that are unpublished, as the unpublished paper being referred to is simply the methodology used to make the calculation and does not contain the data itself - which is publicly available. The new unpublished methodology is a modification of the old method to improve its accuracy to adjust the figures to take account of women who have more than one diagnosis of breast cancer. As such its aim is to ensure the lifetime risk is a conservative calculation and not in any way alarmist. Every year we update our statistics website with the latest UK cancer incidence figures as quickly as we can.
As we explained in our earlier comment, the new 2008 incidence figures for breast cancer changed the lifetime risk from 1 in 9 to 1 in 8 and, as such, it was necessary to publically share this ahead of the methodology being peer reviewed and published. It was imperative to publicise the change widely to ensure both the public, and those working in the cancer sector, had the most up to date lifetime risk figure. Crucially, whether you use the new method or old method, it results in the same overall life time risk. Tthe current established method to calculate life time risks for all cancers is Esteve (1994).
The issue of overdiagnosis and screening is more complex. Screening increases incidence by diagnosing cancers earlier (both in time and at a younger age) than they would otherwise be diagnosed. The vast majority of what is commonly considered 'overdiagnosis' are DCIS cases, and these were not included in the analysis. There are some cancers that would never be diagnosed without screening (and estimates of this are difficult to calculate and vary widely).
The biggest impact will be when screening is first introduced, but the reduced incidence resulting from having found the cancers previously is only apparent once a woman stops being screened. As we keep increasing the upper age of breast screening, we are increasing the incidence in screening age-groups without yet seeing decreased incidence in those screened in the past (and no longer screened).
Our method of calculation only includes malignant cancers, DCIS (in situ) tumours are not included – the only screen detected cancers used in the lifetime risk calculations are those that are invasive. At present the 1 in 8 figure using this more conservative method is best estimate available.
A final point. We mentioned lifestyle risk factors in the press release not as an attempt to account for the increase in the figures, but rather to answer the questions many women have when confronted with stories such as this – namely, ‘what can I do about it?’. The risk of many cancers, including breast cancer, is strongly linked to lifestyle, and it would have been remiss of us not to have included this information in our release.
Dora (not verified) wrote,
Sat, 12/02/2011 - 11:12
As Evan Harris shows the CRUK website attributes the recent steep rise in rates for women aged 65-69 to screening, but Catherine Thomson implies that this is due to DCIS. Contrast this with what the US National Cancer Institute (www.cancer.gov) says about the increase due to invasive cancer following the introduction of screening:
"In addition, investigators differ in their assessments of overdiagnosis regarding how and whether to adjust for characteristics such as lead-time bias.[18,19] As a consequence, the magnitude of overdiagnosis due to mammographic screening is controversial, with estimates ranging from 7% to 50%.[18-21]
Dora (not verified) wrote,
Sat, 12/02/2011 - 11:13
comment continued:
Several observational population-based comparisons consider breast cancer incidence before and after adoption of screening.[22-26] If there were no overdiagnosis—and other aspects of screening were unchanged—there would be a rise in incidence followed by a decrease to below the prescreening level, and the cumulative incidence would be similar. Such results have not been observed. Breast cancer incidence rates increase at the initiation of screening without a compensatory drop in later years. For example, in Sweden, the age-specific incidence rates doubled between 1986 and 2002 for all age groups participating in screening.[22] Another study in 11 rural Swedish counties showed a persistent increase in breast cancer incidence following the advent of screening.[23]
Dora (not verified) wrote,
Sat, 12/02/2011 - 11:17
Comment continued (part 3)
A population-based study from Norway and Sweden showed increases in invasive breast cancer incidence of 54% in Norway and 45% in Sweden in women aged 50 to 69 years, following the introduction of nationwide screening programs.
Dora (not verified) wrote,
Sat, 12/02/2011 - 11:20
Part 4
No corresponding decline in incidence in women older than age 69 years was ever seen.[27] Similar findings have been reported from the United Kingdom [24] and the United States.[25,26]"
References
18) Duffy SW, Lynge E, Jonsson H, et al.: Complexities in the estimation of overdiagnosis in breast cancer screening. Br J Cancer 99 (7): 1176-8, 2008. [PUBMED Abstract]
19) Gøtzsche PC, Jørgensen KJ, Maehlen J, et al.: Estimation of lead time and overdiagnosis in breast cancer screening. Br J Cancer 100 (1): 219; author reply 220, 2009. [PUBMED Abstract]
20) Gøtzsche PC, Nielsen M: Screening for breast cancer with mammography. Cochrane Database Syst Rev (4): CD001877, 2006. [PUBMED Abstract]
21) Zackrisson S, Andersson I, Janzon L, et al.: Rate of over-diagnosis of breast cancer 15 years after end of Malmö mammographic screening trial: follow-up study. BMJ 332 (7543): 689-92, 2006. [PUBMED Abstract]
Dora (not verified) wrote,
Sat, 12/02/2011 - 11:20
part 5
22) Hemminki K, Rawal R, Bermejo JL: Mammographic screening is dramatically changing age-incidence data for breast cancer. J Clin Oncol 22 (22): 4652-3, 2004. [PUBMED Abstract]
23) Jonsson H, Johansson R, Lenner P: Increased incidence of invasive breast cancer after the introduction of service screening with mammography in Sweden. Int J Cancer 117 (5): 842-7, 2005. [PUBMED Abstract]
24) Johnson A, Shekhdar J: Breast cancer incidence: what do the figures mean? J Eval Clin Pract 11 (1): 27-31, 2005. [PUBMED Abstract]
25) White E, Lee CY, Kristal AR: Evaluation of the increase in breast cancer incidence in relation to mammography use. J Natl Cancer Inst 82 (19): 1546-52, 1990. [PUBMED Abstract]
26) Feuer EJ, Wun LM: How much of the recent rise in breast cancer incidence can be explained by increases in mammography utilization? A dynamic population model approach. Am J Epidemiol 136 (12): 1423-36, 1992. [PUBMED Abstract]
27) Zahl PH, Strand BH, Maehlen J: Incidence of breast cancer in Norway and Sweden during introduction of nationwide screening: prospective cohort study. BMJ 328 (7445): 921-4, 2004. [PUBMED Abstract]