Britain’s record on cancer: who’s right?
Claims made by David Cameron and Andrew Lansley about cancer care in the NHS have generated a row that shows no sign of diminishing.
Fresh fuel was thrown on the flames last week by a study reported in The Guardian. The findings, the paper said, challenged the Government’s claims that NHS failings contribute to 5,000 – 10,000 unnecessary cancer deaths a year. It quoted one of the authors, Professor Colin Pritchard of the University of Bournemouth: “These results challenge the feeble justification of the government’s changes (to the NHS) which appear to be based upon overhyped media representation rather than hard comparable evidence.”
It depends entirely which evidence you choose. Professor Pritchard and co-author Dr Tamas Hickish in the British Journal of Cancer (1) chose to focus on mortality data showing reductions in cancer death rates in England and Wales between 1979 and 2006 to match or exceed those of a list of comparator countries. The NHS performance, relatively poor in 1979, has improved more rapidly than that of others.
This, however, does not disprove the central assertion made by the Government, which is that NHS performance, though better than it was, still lags other countries. Nor does Professor Pritchard himself deny this. In another paper (2) in The Journal of the Royal Society of Medicine, also published this year, he concludes: “It must not be forgotten that despite the UK having among the biggest reductions in mortality, UK adult rates are fifth highest among Western countries and their older rates sixth highest, so there are no grounds for complacency ...” When talking to The Guardian this reservation seems to have been forgotten, or went unreported.
The Government’s claims are actually based on the numbers who survive cancer rather than the numbers who die. The most recent comparison comes from a team lead by Professor Michel Coleman of the London School of Hygiene and Tropical Medicine, whose report in The Lancet earlier this year (3) included among its authors the National Director for Cancer, Professor Sir Mike Richards. The conclusion was that survival had improved in all the countries studied, but was persistently higher in Australia, Canada and Sweden, and lower in Denmark, England, Northern Ireland and Wales.
For example, one-year survival in colorectal cancer in 2005-07 was 84.9 per cent in Australia, 83.5 per cent in Canada, 82.4 per cent in Norway, and 83.8 per cent in Sweden. But in Denmark it was 77.7 per cent, and in the UK 74.7 per cent. Comparable gaps were found for five-year survival, and also applied to lung, breast, and ovarian cancer.
Two years ago Professor Coleman and colleagues calculated how many deaths this gap in survival might cause (4). The calculations showed that had the NHS achieved average European performance, 6,600-7,500 premature deaths a year could have been avoided between 1985 and 1999. Matching the best European survival rate would have prevented around 12,000 deaths a year.
On this basis, David Cameron and Andrew Lansley were entitled to make the claims they did. Considerable improvements notwithstanding, the UK does, or did, still lag some way behind other comparable countries. There is, however, a difference of academic opinion over whether survival data are reliable enough to prove the case. An editorial in BMJ advancing this view (5) was rebutted by Professor Coleman, who called it “unfounded, untenable and inconsistent”. BMJ has since published another paper from Professor Coleman’s group giving chapter and verse (6).
So the veracity of the Government’s claims depends largely on which expert you choose to believe. A subsidiary argument, advanced in the recent Pritchard paper is that pound for pound the NHS has done better than any other system in cutting cancer deaths.
That is probably true, but it may also explain why gaps remain. The NHS is a relatively cheap system because GPs restrict access to specialists. That means that cancer referrals are often delayed, which in turn leads to worse outcomes. So the very factor that makes the NHS more affordable also militates against the early diagnosis of cancer. GPs see only a handful of new cases a year, and are under pressure to limit referrals. They are not experts in cancer diagnosis and often delay sending patients to specialists, who are.
It is interesting that Denmark, which also has relatively poor performance, is similar to the NHS in employing GPs as gatekeepers. A study by two Danish researchers from Aarhus University published in the British Journal of General Practice in August (7) found that systems with a strong gatekeeper function do tend to show worse one-year survival for cancer. Poorer survival at one year is likely to translate into poorer survival overall.
If this is so, then the NHS may never be able to match the performance of systems in which worried patients refer themselves directly to specialists. That conclusion may be unpalatable, but is consistent with the evidence.
References
- C Pritchard and T Hickish, British Journal of Cancer, online publication 4 October 2011
- C Pritchard and M S Wallace, J R Soc Med Sh Rep 2011;2:60
- M P Coleman et al, The Lancet, 377: 9760; 127-138, 8-14 January 2011, accessible here
- M Adbul-Rahman, MP Coleman et al, British Journal of Cancer (2009) 101, S115- S124
- Valerie Beral and Richard Peto, BMJ 2010; 341: c4112
- Laura Woods, MP Coleman et al, BMJ, 2011; 342: d3399
- Peter Vedsted and Frede Olesen, Brit J Gen Pract 2011, Aug 61 (589) 508-512
Update:
Laura Woods and Michel Coleman of the London School of Hygiene and Tropical Medicine have provided an interesting comment which I am attaching to the article as it includes a graph which cannot be displayed in the normal comment box: Their comment follows:
If cancer mortality trends were the most appropriate basis for assessing the performance of health services, the NHS would have been shut down long ago for lethal sex discrimination (Figure).
The death (mortality) rate for lung cancer in men, adjusted for changes in the population age structure over time, has fallen rapidly over the past 30 years from around 100 per 100,000 per year in the early 1980s to around 50 per 100,000 in 2008. In women, the lung cancer death rate has increased from 28 to 30 per 100,000 over the same period. If we presented this as a 7% rise in the lung cancer death rate for women but a 50% drop for men, every politician in the country would be asking: why has the NHS become steadily worse at treating women with lung cancer for the last 30 years, but so much better at treating men?
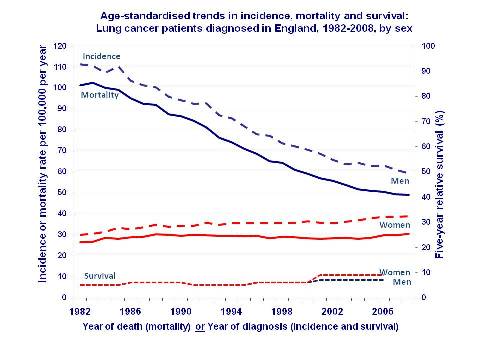
The answer, of course, is that the data have been woefully mis-interpreted. Lung cancer death rates are rising in women because more women are getting the disease (higher incidence rate). In men, by contrast, the incidence rate has fallen rapidly, leading to a big drop in the death rate. Crucially, five-year survival from lung cancer has remained stubbornly constant at around 10% throughout the entire 25-year period 1980-2005 – and survival is the same in both sexes. The correct interpretation of these data is simple: the outcome for lung cancer patients has barely improved at all since the early 1980s, and the starkly contrasting changes in lung cancer death rates in men and women have been driven almost entirely by changes in the incidence rate. In turn, this is because men have progressively stopped smoking since the 1950s and women (broadly speaking) have not. In short, the lung cancer mortality trends have little or nothing to do with the performance of the NHS.
Politicians of all parties regularly abuse health data for their own purposes. For example, we are not aware of any evidence that the radical reform of NHS structure currently under parliamentary debate will improve cancer survival. We are not saying it won’t, just that it is dishonest for those pushing for change in the NHS structure to claim that it will, and that the reforms are justified for that reason. Cancer survival is high in the USA, where the health service structure is more similar to that proposed in the NHS reform, but it is also high in Sweden and Finland, where the health service is more similar to the NHS as it is today.
Two issues have arisen in this debate: first, whether survival or mortality data should be used to assess progress against cancer, and second, whether cancer registration data are of sufficiently high quality to enable reliable assessment of cancer survival.
The answer to the first question is that all three measures: incidence, mortality and survival – are required for reliable evaluation of progress in cancer control. This is clearly illustrated in the lung cancer example given here. It makes no sense to rely exclusively on mortality trends and to ignore the trends in how many people get the disease in question (incidence) and the trends in survival after it has been diagnosed. If patients are gradually being diagnosed at an earlier stage of disease but the outcomes do not improve, survival times will still be longer, but that type of increase in survival can be spotted from a rise in incidence with no change in the death rate. Monitoring the trends in survival alongside the trends in incidence and mortality provides a very good indication of progress in health service performance and in wider cancer control. Monitoring cancer mortality rates alone does not.
We answered the second question in what you describe as the ‘chapter and verse’ paper published in the British Medical Journal (BMJ) earlier this year. We considered in that paper whether the cancer registry data used to create survival statistics are sufficiently reliable. We showed that the errors that had been suggested in a BMJ editorial in 2010 as making UK survival statistics unreliable cannot in fact explain the differences in cancer survival between (say) Sweden and the UK.
We will publish soon a fuller explanation of the relationship between incidence, mortality and survival in an attempt to clear up the persistent confusion. Until then, we repeat here the conclusion of our BMJ paper: “The question has long since ceased to be whether such unacceptable differences in cancer survival exist. The question is what the underlying mechanisms are, and what can be done to improve the outcomes for patients with cancer in the UK.”
Dr Laura M Woods
Professor Michel P Coleman
Cancer Research UK Cancer Survival Group
London School of Hygiene and Tropical Medicine

Mike O'Neill (not verified) wrote,
Wed, 16/11/2011 - 09:01
This area is a very good example of how you can can prove just about anything with statistics by being selective with the data you choose or how you present it. And how difficult it is to be truly objective. Earlier diagnosis will, by definition, lead to increased survival times even if outcome is not affected by how early treatment is given. Earlier diagnosis also probably leads to increased misdiagnosis and so part of any increased survival times may be due to including some people who did not have the disease in the first place. Countering that, earlier diagnosis almost certainly does lead to longer survival in at least some patients.
I have not seen reports of any studies that take all three of these points into account when coming to their conclusions. Are there any?
steve black (not verified) wrote,
Wed, 16/11/2011 - 11:41
Am I missing something clever in the statistical analysis here? I thought that survival rates were a very bad metric for evaluating the effectiveness of care for cancer. A patient whose treatment will make no difference to the date of their death will have a better 5-year survival rate if they are diagnosed early. Only if treatment lowers the overall mortality can we assert that treatment is better; just diagnosing earlier is only good if it also improves mortality.
satish kumar (not verified) wrote,
Mon, 28/11/2011 - 13:15
the fact of the matter no matter how stats are interpreted is that access to cancer treatments in this country has had at least some role in worse survival for many common cancers here, in addition to the inherent limitations in the system with Gp's as gate keepers. We are past masters at fudging issues, if health outcomes are poor in this country, then we question the veracity of information held in tumour registries or the way stats are done, but find it difficult to accept that our health system has just about reached its limits of efficiency in the 21'st century.
ted willis (not verified) wrote,
Sat, 31/03/2012 - 17:41
It is absurd that organisations such as the Commonwealth Fund spend a lot of time and money on detailed comparisons of health care systems - and their findings are ignored, while the NHS is slagged off on the basis of comparisons of cancer survival - which is a very poor measure of healthcare systems - ie all these breast cancer DCIS cases found by screening - improve survival figures but benefit noone as they mostly are insignificant.