Decrease in cocaine-related deaths was in 2009, not 2010
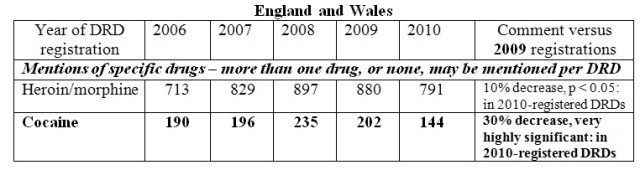
Background: In an article here on 24 August 2011, sub-titled ‘a wake-up call the Registrar General’, I highlighted the trends published by Office for National Statistics (ONS) for England and Wales – which are by calendar year of death-registration – for the following drugs-related deaths (DRDs): a) heroin/morphine-related; b) cocaine-related.
I have since obtained from ONS the corresponding information on DRDs by year of death. This information is presented below for DRDs that were registered within the same quarter-year or subsequent 4-quarters as death occurred. Please notice that my second table begins in 2005 and ends in 2009, and so is shifted by a year; and that the commentary is versus 2008.
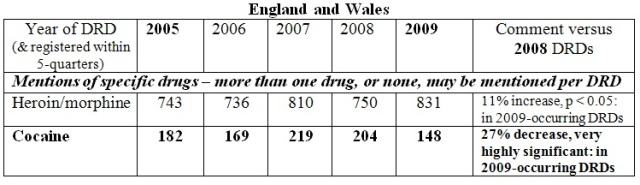
Cocaine-related: the major, highly significant reduction in cocaine-related DRDs actually occurred in 2009 – not 2010. The 2009-decrease clearly accords, in timing, with the major decrease in cocaine-positives in the British Army’s compulsory drug testing programme and, in magnitude, with the evidence from British Crime Survey’s (BCS’s) representatively-sampled householder-interviews in 2010/11.. The 2010/11 BCS’s 16-24 year old respondents’ past-year use of cocaine powder had decreased by 29 per cent compared to the previous two-years’ interviewees: down from 6.2 per cent (95 per cent CI: 5.7 - 6.7 per cent) past-year use to 4.4 per cent (CI: 3.7 - 5.1 per cent).
Heroin-related: Notice that when heroin-related DRDs are viewed by year of death rather than by registration-year, the statistically-significant 10 per cent decrease in registrations in 2010 is revealed as being actually an 11 per cent increase in heroin-related DRDs in 2009 compared to 2008!
When monitoring DRD-epidemics, we simply cannot tolerate 1-year distortions, as above, of actual time-trends which registration-delays, as in E&W, are responsible for. If we are serious about the loss of life-years to heroin and cocaine, then epidemiologically-untenable delays in obtaining the toxicology on suspect DRDs have to be addressed.
Am I riding a hobby-horse on death registrations: And is it time that I dismounted? Indeed I am, and I don’t intend to come off until the registration-problem is resolved.
Another correspondent has rightly remarked that properly determining cause of death has to await the coroner’s verdict. Indeed so, but . . . toxicology is more important that ICD-10 code when considering DRDs. For 90 per cent of DRDs, toxicological classification should surely be available within 3-months – that is, in the same or subsequent-quarter as death?
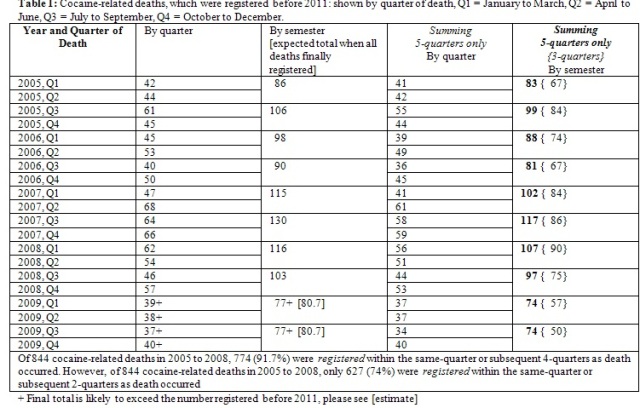
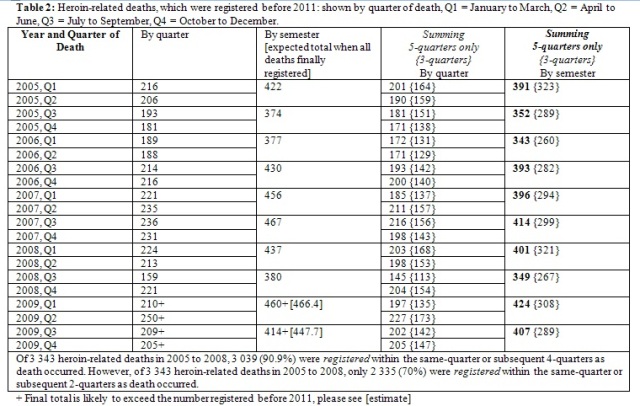
Supplementary tables below show that it is not until 5-quarters have elapsed that we can be sure that 90 per cent of DRDs have been registered. And that only 70 -75 per cent are registered in the same or 2-subsequent quarters as death occurred.
Little wonder, then, that epidemiological trends can be out by a year if assessed by the (distorting) time-scale of registration rather than by the relevant time-scale of when death actually occurred.
What needs to be done? First, Office for National Statistics should please routinely provide additional published tables on DRDs by year of death – as they have kindly done for me on request. In the first instance, as here, ONS may need to adopt a policy of basing year-of-death inferences on DRDs which were registered in the same quarter or 4-subsequent quarters as death occurred.
Second, there needs to be registration of the fact of death within 8 days of ascertainment of any death; and a facility for ONS to be able to identify deaths which were subject to coroner’s autopsy.
Third, UK needs a toxicological protocol for the investigation and reporting of suspect DRDs - nearly all of which are subject to coroner’s autopsy - so that the toxicology on suspect DRDs is available within 3-months for at least 90% of all suspect DRDs.
Fourth, there needs to be timely analysis of the toxicology on suspect DRDs – both to inform decisions by UK’s Advisory Council on the Misuse of Drugs and to show young people and their families that the public health takes very seriously indeed the toll of lost life-years that addictions claim.
Fifth, I appeal to UK Statistics Authority, National Statistician, Chief Medical Officer, Health Secretary, Justice Secretary, and Home Secretary and their key advisers to bring their redoubtable intellectual, practical and policy resources to bear on this cross-departmental issue.
Conflicts of interest: SMB writes in a personal capacity but currently serves on Home Office’s Surveys, Design and Statistics Subcommittee and on UK’s Scientific Pandemic Influenza Advisory Committee and, in 2010, was a member of Chief Medical Officer’s H1N1 Statistical Legacy Group and, on behalf of the Royal Statistical Society, gave evidence to the Science and Technology Select Committee’s Inquiry into Scientific Advice in Emergencies.
Acknowledgement: SMB gratefully acknowledges Patrick Mercer OBE MP whose written parliamentary questions crucially elicited the quarterly results on cocaine-positivity in the British Army’s compulsory drugs testing programme.

Chris Taylor (not verified) wrote,
Mon, 19/09/2011 - 10:12
"Decease in cocaine-related deaths"...?
misterjohn (not verified) wrote,
Mon, 19/09/2011 - 23:58
Try proof reading the title of your article. If that can't be got right, why should we believe the rest of the information?
Nigel Hawkes (not verified) wrote,
Tue, 20/09/2011 - 08:03
Thanks foir pointing that out - now correected, with apologies