Drugs deaths in England and Wales - a wake-up call to the Registrar General
Yesterday's report on Deaths Related to Drug Poisoning in England and Wales 2010 by the Office for National Statistics (ONS) risks a charge under the Trade Descriptions Act.
Its proper title ought to be Deaths Related to Drug Poisoning in England and Wales registered in 2010.
That would more accurately describe its contents, for many of the deaths reported on will have occurred in 2009. In addition, many drug-related deaths (DRDs) which occurred in the last quarter of 2010 may – as yet – be unknown to ONS if the coroner to whom the death was referred has not reached his/her verdict on the cause of death. This lacuna in England’s registration of deaths shames us all – that, in the 21st century, England cannot properly count its dead.
Worse, because there is no requirement for timely registration of the fact of death, we don’t even know how many deaths we are lacking cause-of-death information for. What sort of accounting system is that – when coroners’ delays cannot even be properly measured?
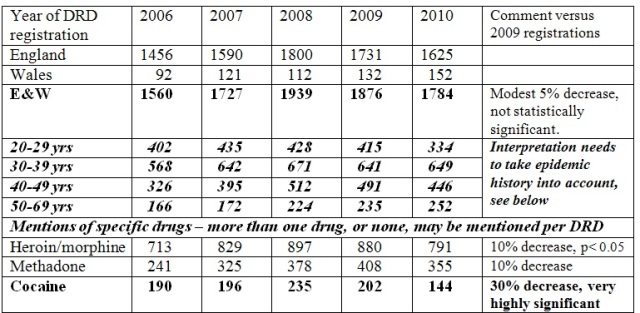
What are the registration-scrambled messages on DRDs in England and Wales? Several are summarised in my Table, which uses ONS’s drug misuse definition as recommended by Advisory Council on Misuse of Drugs (ACMD). Anticipated by Straight Statistics and consistent with the British Crime Survey’s interviews about cocaine use in 2009/10, there is a highly significant decrease in cocaine-related DRDs. However, yet to be identified is the semester in 2008 or 2009 from which the decrease in cocaine-related deaths was first evident
 .
.
Historically, England and Wales have had an epidemic of heroin use by injection and many of today’s DRDs are the result as this wave of heroin-injectors ages. More recently, in the mid 1990s and into this century, an epidemic of cocaine use has been documented by British Crime Survey (BCS) until, in 2008, mephedrone came on the scene. The BCS interviews in 2010/11 recorded a major decrease in past-year use of cocaine relative to interviews in two previous years. To an opium crop failure in Afghanistan we may owe the 20 per cent decrease in Scotland’s heroin-implicated deaths in 2010 – more modest in England and Wales where, unlike Scotland, the decrease in registered methadone deaths was of a similar order.
In 2010/11, the Welsh Assembly had supported an evaluation of take-home Naloxone, and will hope that, from 2010, its heroin-implicated DRDs (by date of death) might be lower than otherwise expected . . . far too soon to know. Indeed, even a real decrease of a quarter in Welsh DRDs would have to be reckoned over a 3-year period, or longer.
With so many different factors to conjure with when analysing DRDs, it is little wonder that ONS, like the rest of us, is hampered by use of the wrong time-scale: the year of registration of death, rather than the year of occurrence. Until the Home Secretary (who is ultimately responsible) and Parliament bring England’s registration of deaths up to date, the best that ONS could do is to publish supplementary tables by year of death. That would show just how much registration delay confounds DRD-analyses.
DRD-tables by year of death would, of course, run a year late because ONS does not have a nearly-complete account of all DRDs which occurred in any given year, until almost 18 months later. For 2009, that would be at its May 2011 data-freeze.
I say “nearly-complete” because, on page 6 of the new report, ONS politely points out another problem that it should not have to contend with. “In around 12 per cent of drug poisoning deaths only a general description is recorded on the coroner’s certificate of death (such as drug overdose or multiple drug toxicity)” it reports.
In other words, not only is the registration of deaths delayed for months to allow for the coroner’s verdict, but when those verdicts finally emerge one in eight of them is apparently so ill-defined that the DRD cannot be classified by toxicology.
Do we care? Are we sufficiently serious about tackling the dreadful loss of mainly young lives to DRDs? Or, do they matter so little that the Home Secretary (who is ultimately responsible for the office of the Registrar General) and Parliament continue to be satisfied by data which are on the wrong time-scale for epidemiologically insightful analysis and, for 1 in 8, lacking in an adequate toxicological account?
Conflict of Interest: SMB writes in a personal capacity. She also serves on Home Office’s Surveys, Design and Statistics Subcommittee.

Mike O'Neill (not verified) wrote,
Thu, 25/08/2011 - 08:25
Does Sheila Bird really want coroners to provide cause of death before they know what it is? That seems to be what she is asking for.
Allocating cause of death to the actual year of death might improve the quality of the statistics when looking at long-term trends but has the disadvantage that initial reports would have a category of 'not yet known' and so initial analyses would be subject to change. So whether 'year-by-year as reported' or 'year-by-year as occurred' is better will be a matter of judgement; some will prefer one, some will prefer the other.
It might be good to know whether Coroners Court decisions are getting faster or slower to reach the statistics but is surely a minor consideration in how the statistics are presented.
This is a hobby horse that Ms Bird needs to get off.
Reevel Alderson (not verified) wrote,
Thu, 25/08/2011 - 08:53
This is an interesting report, coming just eight days after the publication of the figures for Scottish drug-related deaths http://www.gro-scotland.gov.uk/files2/stats/drug-related-deaths/2010/dru.... Statisticians cautioned it was too early to say if the reduction in the number of DRDs in the past two years was a trend; they said a three-year reduction would be needed before that could be declared. Drugs workers, including those at the Scottish Drugs Forum, say the high number of DRDs in Scotland could in part be due to the rigourousness of data collection. But others, notably Dr. Roy Robertson a GP in Edinburgh and academic at Edinburgh University, argue the published figure is too low. If deaths from drug-acquired HIV and Hepatitis-C were included, along with road deaths caused by a driver under the influence of drugs, the real drugs-related death toll in Scotland would be even higher. Reevel Alderson, Home Affairs Correspondent, BBC Scotland.