Swine flu data: through a glass darkly
By 16 December 2010, there were 182 patients with swine flu in intensive care units in England, equalling the worst week in 2009 (180) and deaths from H1N1 had risen from 10 (when doctors first drew public attention to the toll among the under-65s) to 17.
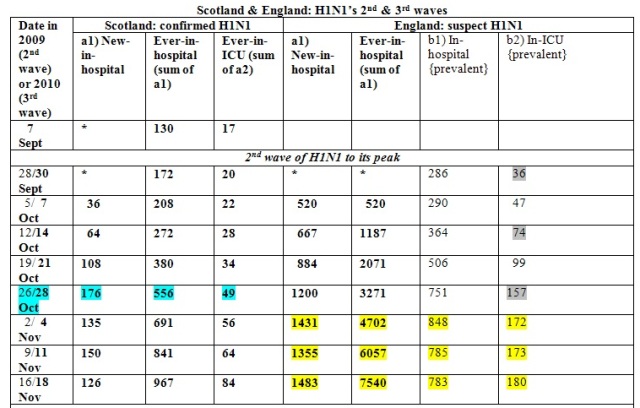
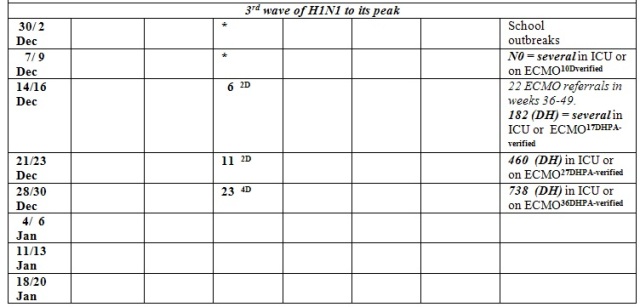
Since then, as my Table shows, prevalent ICU admissions for H1N1 have doubled on a weekly basis (182, 460, 738) and stood at 738 when announced by Department of Health on 30 December – that is, four times the peak in 2009. Verified H1N1-deaths, which are an under-count (see below), have increased on a slower trajectory (10, 17, 27, 36).
Comparing the second and third waves of H1N1, the first thing to notice is the dearth of hospitalization data for severe H1N1 cases in this current outbreak. Secondly, we should be concerned that the doubling-time for England’s prevalent ICU cases of H1N1, which was roughly 2-weekly (see grey shading: 36, 74, 157) in the second wave, is currently weekly (182, 460, 738).
However, during Scotland’s second and third waves of H1N1, its ever-ICU admissions initially doubled on weekly basis: the second wave as 3 {= 20-17}; 5; 11; 17; 32; and thereafter more slowly: 39 {= 56-17}; 47 and 67 and the third wave as 6; 11; 23; to be continued.
Finally, the reported death-rates between Scotland (for ICU-admissions only) and England (verified H1N1-related) are grossly non-comparable - presumably because of under-counting in England as Scotland’s ICU-death-rate is comparable with that reported from Australia & New Zealand during their 2009 winter-season of H1N1.
What should be reported in this third wave of H1N1, as a legacy of what we learned in the two earlier phases? So far, and unlike in 2009/10, the Health Protection Agency has not properly reported the numbers hospitalized or admitted to ICU by age-group. And press reports have failed to distinguish clearly between
a) The number newly admitted to ICU for suspect H1N1 in the current week (that is: incident admissions), and
b) The number currently in ICU for suspect H1N1 at 10.00hrs on Tuesday in the current week (that is: prevalent admissions): see Table.
By cumulating incident admissions to ICU, we can track publicly how many ICU-admissions there have been for suspect H1N1 since the start of the third wave, presumably some time in late November 2010 in England but perhaps later in Scotland.
By monitoring b) prevalent ICU admissions, we can monitor pressure on ICU capacity.
During the second wave of swine-flu in 2009/10, there was weekly age-group-specific reporting on both a) and b) and also regular reporting of the number of H1N1-related fatalities – although not by the week of the death’s occurrence. The Chief Medical Officer’s Statistical Legacy Group, set up after the first waves of H1N1, hoped that this style of reporting would be available in time for further pandemic monitoring – but so far it is not. And please may we have a common reporting site for ALL key surveillance data on H1N1.
Instead, as my Table shows, the surveillance trough is half empty – thanks to a delayed start to public reporting on the third wave; a lack of clarity from the Health Protection Agency and Department of Health, and accordingly also the press, about which of a) or b) is being reported; no common site for comprehensive situation reports on H1N1 epidemic (not a good advertisement for Public Health England); and no attempt to attribute reported H1N1-related deaths to their week of occurrence. Delays in the notification of deaths, as CMO Statistical Legacy Group pointed out, seriously hinder the proper monitoring of the most severe consequence of H1N1 – including by age-group.
As for immunisation, claims have been reported that after the first two waves of H1N1, 50 per cent of children are immune . . . but where are the data on which this claim rests? No sensible scientist accepts such a claim without having seen the evidence for it. Both public and independent scientists should have access to the data that appears to be informing public health policy, but at present do not.
The Health Secretary Andrew Lansley reinstated the national advertising campaign, cancelled to save just £600,000, according to The Guardian, or “up to £1 million” according to The Times. At £600,000, the campaign would be cost-effective if it prevented even a single child dying from H1N1.
Immunization of pregnant women is not being universally offered despite the efforts of the acting CMO, Dame Sally Davies. Before Christmas, a friend’s daughter-in-law who is half-way into the third trimester of her first pregnancy was admitted to hospital for several days’ observation of her pregnancy but was not offered immunization until, prompted to do so, she went to her general practitioner to request the vaccine.
SMB writes in a personal capacity but serves on UK's Scientific Pandemic Influenza Advisory Committee and served on CMO's Statistical Legacy Group.
