Outing H1N1 data
Diligent parliamentary questions by Andrew Pelling MP have elicited some useful information on H1N1 flu, which deserve a wider public.
Two or three times a year, the Royal Statistical Society offers a statistical seminar for journalists at which it also welcomes press officers, members of parliament and their researchers. Andrew Pelling’s parliamentary researcher attended our June 2009 seminar.
Mr Pelling, MP for Croydon Central, has since tabled some well-informed parliamentary questions to obtain information on the incompleteness of quite basic data on UK’s virologically confirmed H1N1 cases up to 16 June 2009. There were 1,052 such H1N1 cases in England, Wales and Northern Ireland. For full details, click here.
QUESTION A. Mr Pelling asked: for what proportion of these 1,052 H1N1 cases was the start-date of H1N1 antiviral treatment or prophylaxis known.
ANSWER A. ‘Complete data on the commencement of antiviral or prophylaxis is not known. This is because once detailed data on the first few hundred cases had been collected, the Health Protection Agency (HPA) stopped collecting that level of detailed information’.
Comment: Why did HPA not volunteer to provide the relevant information on treatment/prophylaxis for the ‘first few hundred cases’ (how many are they, exactly?) on whom it claims to hold ‘detailed data’. Follow-up parliamentary questions are needed to achieve transparency.
QUESTION B. Mr Pelling asked: how many of the above 1,052 H1N1-confirmed cases were recorded as having been hospitalized by 30 June 2009; and for the age-distribution of the hospitalized cases.
ANSWER B. ‘Not all of the requested data are currently available. Verified data on hospitalizations is only available up to 16 June 2009.’
Comment: Not good enough! How can we confidently work out the 2-week H1N1-related hospitalisation rate by age-group except by comparing the age-distribution for all 1,052 H1N1 cases (confirmed by 16 June) with the age-distribution for the subset of them who were hospitalized by 30 June 2009? These data are utterly crucial because, from 2 July 2009, virological confirmation of suspect H1N1 cases ceased.
Follow-up parliamentary question are thus needed. Firstly, to establish if the hospitalization rates to 30 June 2009 (by age-group) for the above 1,052 cases have since been ascertained. Secondly, to establish by age-group the hospitalization rates by 14 July 2009 for the 4,000+ H1N1 cases in England, Wales and Northern Ireland who were virologically confirmed between 17 and 30 June 2009.
These 4,000+ cases are virtually the last major virologically-confirmed H1N1 case-cohort for whom we can actually have hospitalization rates for the simple reason that routine H1N1 virological confirmations were suspended soon after 30 June 2009.
Drift in age-distribution, and hospitalization rates by age-group, between Mr Pelling’s initial cohort of over 1,000 H1N1 cases and the suggested follow-on cohort of over 4,000 H1N1 cases is fundamentally important UK-specific information. Where are the data?
QUESTION C. Mr Pelling also elicited very basic information on the above 1,052 H1N1 cases by asking that they should be cross-classified by H1N1-exposure (imported, indigenous, and unknown which applied for 422/1,052 = 40 per cent), sex (male, female, or unknown, which applied for 94, 9 per cent), and age-group (under 10 years, 10-19, 20-29, 30-39, 40-49,50-59, 60+, or unknown which applied for 107, 10 per cent). He also elicited the age-distribution for H1N1 cases according to whether or not their date of symptom onset was known (unknown for 556, 53 per cent).
ANSWER C. The information gleaned is summarized below. For full details, follow this link.
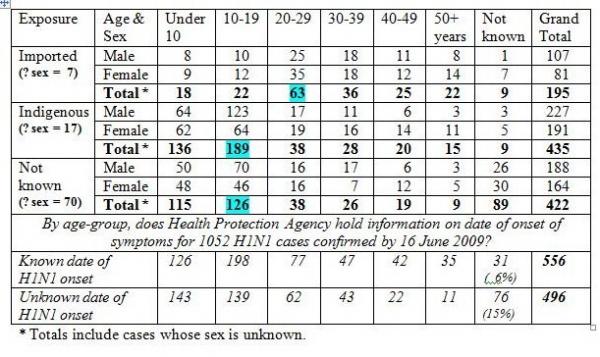
Comment: First, as anticipated, the modal age-group (highlighted in green) is older for imported (20-29 years) versus other H1N1 cases (10-19 years). In particular, only 18/184 (10 per cent) of known-age imported cases of H1N1 were under 10 years of age, but significantly higher proportions are found in known-age indigenous cases (136/426, 32 per cent) and those whose route of exposure was unknown (115/333, 35 per cent).
Second, most H1N1 cases whose exposure is recorded as ‘not known’ are probably indigenous - both because travel history should have been easy to elicit and similarity of known-age-distributions.
Third, ‘missingness’ mingles. Thus, information on age was absent for 15 per cent of the 496 H1N1 cases whose date of symptom onset is missing but for only 6 per cent of those whose symptom onset was ascertained. Onset date was unknown for a high proportion, 53 per cent, of H1N1 cases under 10 years of age (143/269), for 41 per cent of known-age H1N1 cases aged 10-19 years (139/337) or older (138/339), but for the vast majority, 71 per cent, of the 107 H1N1 cases with unknown age.
Although I knew these answers on data quality, I could not have put them into the public domain as quickly as Mr Pelling did because the Health Protection Agency requires 30 days to vet analyses – be they basic or complex - before they can even be submitted for publication.
WHAT NEXT? We must hope that Mr Pelling can repeat his set of parliamentary questions for the next cohort of 4,000+ H1N1 cases in England, Wales and Northern Ireland virologically-confirmed between 17 and 30 June 2009. Has there been further drift in the age-distribution of now-mostly-indigenous H1N1 cases? Critically, we need to assess, by age-group, hospitalization rates within 2 weeks of H1N1 case confirmation. We shall not ever have this information for H1N1 cases in July 2009 because routine virological confirmation was suspended on 2 July.
Mr Pelling, bully for you; and please continue your questions . . .
(Sheila Bird is Vice-President of the Royal Statistical Society.)

Deborah Stanford (not verified) wrote,
Wed, 22/06/2011 - 08:51
From a behavioral view I find the mass media attention in the flu virus interesting and also dangerous. I personally saw a large government department devote more than six months and just about its entire workforce were working on policy to restrict the influenza virus entering their environment.
Deborah
http://psychologycareerhq.com/