The perverse results of the 18-week wait
This week the Government’s full response to the Future Forum, set up to rescue the health bill, made it clear that the NHS Constitution is to be reinforced. Everybody who works in the service is enjoined to treat it with due deference and ensure it informs their every action.
Among the items spelled out in the constitution is a patient’s right to treatment by a hospital specialist within 18 weeks’ of referral by a GP. It is one of only two such waiting-list guarantees written into law as a result of the Health Act 2009 (the other is the maximum two-week wait for a cancer appointment deemed urgent by the GP.)
Was it wise to enshrine the 18-week wait in law? All targets distort behaviour, and there is plenty of evidence this one has. NHS waiting lists are a playground for connoisseurs of statistical witchcraft: they almost always seem to say something that, on close examination, they are not saying at all.
The 18-week wait was deemed an impossible dream when first proposed by the Labour Government, but it was nonetheless achieved in 2008 to widespread acclaim. The Coalition Government, though opposed to targets, retained it, and in its response to the forum has reaffirmed it.
The target is being met, so would it be safe to assume that nobody is waiting for more than 18 weeks? Hardly. The target actually says that 90 per cent of patients have to be seen within 18 weeks, which enables trusts to keep the other 10 per cent waiting much longer. I’m obliged to an excellent blog on the Health Service Journal website for the information in this post. The blog is written by Rob Findlay, and is also accessible on his own website.
It may seem surprising that two years after achieving the 18-week wait, there are still patients out there who have been waiting more than 52 weeks for treatment. Paradoxically, the target works to the disadvantage of these patients, because although they do show up in other waiting-time statistics, attention tends to be focussed on the 18-week one. So long as nine out of ten patients are treated within 18 weeks, the target is met. There is therefore a perverse incentive for trusts to ensure that for every ten patients treated, nine are short-waiters, and only one is a long waiter.
That means that once their wait exceeds 18 weeks, patients’ chances of an early appointment could tend to diminish rather than increase. Rather than hurrying to tidy up the long tail of patients kept waiting for ages, as you might expect, trusts are incentivised to ignore them as much as they can and only offer them appointments in carefully-calculated numbers. Is this happening? Given the near-legendary skill of NHS managers to “game” targets, and the mass of data assembled from NHS sources by Mr Findlay, it appears that it is.
In April 2011, the most recent figures available, there were 236,155 patients who had been waiting more than 18 weeks. This is 9.5 per cent of the total, so the target was met. The number waiting more than 18 weeks has changed relatively little for the past two years – in April 2009 it was 250,509. Some have waited a very long time indeed. In April 2011, there were 14,435 patients who had waited more than 52 weeks.
Data by trust show big variations. University College Hospital in London meets the 18-week target easily, but has a very long tail of patients waiting longer than that. One in ten of these have waited longer than 42 weeks. Kingston Hospital NHS Trust is in a similar position.
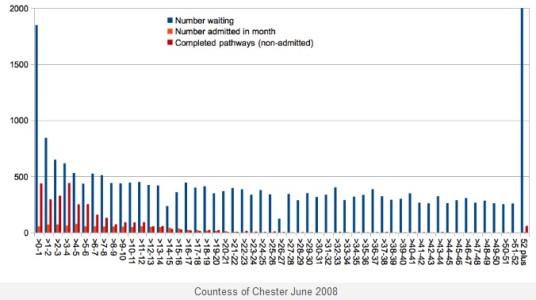
An extreme example, again taken from Mr Findlay’s blog, is that of the Countess of Chester Hospital in June 2008 (below). At the time it was meeting the 18-week target, but nonetheless had 17.943 patients waiting more than 52 weeks – the bar on the extreme right which, if drawn to scale, would go way off the chart. (This is illustrative of the possibilities, and not intended to point the finger at Countess of Chester. Many other trusts were in a similar position at the time.)
The dilemma faced by trust boards is exemplified by a quotation from the board minutes of Portsmouth Hospitals NHS Trust at its May meeting. This recorded that at the end of March there had been 1,319 patients in the over 18-week backlog and it had been agreed to make an effort to clear it. The result, inevitably was a “deterioration in our performance against the 90 per cent target for admitted patients”.
So trying to do the right thing by patients meant the trust was risking breaching the 18-week guideline, which now has become a target that cannot be missed. Trusts that do miss it risk substantial fines.
It would be possible, technically, for the backlog to get bigger and bigger without this central target being breached. So for an important minority of patients, the preferred target acts against their best interests. It is unclear even how many members of trust boards are aware of the issue: Mr Findlay studied the data given to board members by scanning trust websites, and found that all, or almost all, were given figures on whether the trust had achieved the 18-week target, but only a quarter saw data on patients whose pathways were incomplete – that is, they had been referred but not seen. He reckons nearly half trusts do not provide data to their boards about patients who are still waiting – unless they do so in private session unrecorded in the minutes.
He concludes: “There are currently eight measures of waiting times in common use at English acute Trusts. Bizarrely, a trust can meet six (and in the short term seven) of these measures, cost-free, by refusing to treat any patient who was referred more than 18 weeks ago.”

Rich (not verified) wrote,
Fri, 24/06/2011 - 09:15
So a tactical response by patients would be to ask their Doctor to re-refer them after 20 weeks. Is that possible? What would happen to the targets then?
CL (not verified) wrote,
Fri, 24/06/2011 - 09:15
This article makes the important point that targets (or legal constraints) distort behaviour. They are of course intended to influence behaviour, in this case reducing the proportion of people waiting over 18 weeks, so not all effects are perverse. To be fair, you cite a Trust where this perverse effect has been acknowledged and an attempt made to reduce the backlog, so there is evidence that the backlog is not always the result of cynical manipulation.
Since an 18-week wait has gone from "an impossible dream" to reality for 90% of patients, we need to balance the perverse consequences against this remarkable benefit. An alternative to abolishing (or re-branding) targets might be to refine them - considering maximum or mean waiting times in addition to existing constraints.