Ten years and too few answers later ...
Ten years ago, the Home Affairs Committee’s Special Report on Drugs and Prisons made a series of recommendations that are still being ignored by the Ministry of Justice.
In its report of January 2000, the committee recommended, inter alia (the bold numbers refer to the relevant paragraphs, while the Government responses are bracketed and italicised):
33. The random Mandatory Drug Tests (rMDT) results provide evidence consistent with a downward trend in the use of cannabis within prison . . . We see no indication that there is any downward trend for use of opiates. {The Government shares the Committee’s view}.
42. We think that further steps may be needed to ensure that the new strategy impacts more powerfully on hard drug use than cannabis use. {The Government shares the Committee’s view but it is far too early to draw conclusions about the effect of the new drug strategy on the use of individual drugs}.
46. We recommend that the Key Performance Indicator (KPI) used for addressing drug abuse be recast in such a way as to give greater emphasis to the fight against harder drugs; this could be done either by setting a target for harder drugs alone, or by setting a separate sub-target for harder drugs within the overall target. {The Government notes the Committee’s view and the Prison Service will consider the creation of a different KPI}.
Ten years on, no separate KPI on opiate-positive rates in rMDT has been adopted. This is scientifically inept because cannabis stays in the urine for 2 weeks, heroin for only 2 to 3 days.
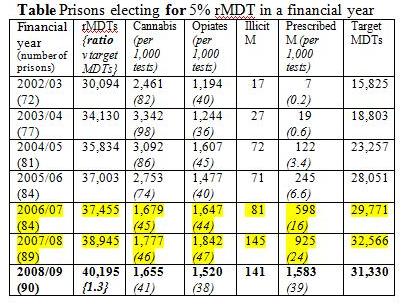
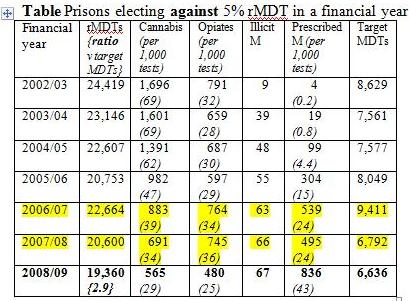
Yet, in January 2010 Maria Eagle, Minister of State at the MoJ, was still ignoring the need to report separately prisons’ opiate positive rate in rMDTs from their cannabis positive rate. Instead, she offered the House the same old story: “Drug misuse in prisons, as measured by random mandatory drug testing, has fallen by 68 per cent since 1996/97”. See Tables for data since 2002-03.
With opiate positive rates this century of around 4 per cent and cannabis positive rates around 8 per cent in prisons opting to test 5 per cent of their inmates (usually the larger jails), around 36,000 rMDTs are needed (and achieved, see Tables) to discern nationally a year-on-year 10 per cent change such as from 40 to 36 opiate positive per 1,000 testees; and 24,000 rMDTs to discern nationally a year-on-year 8.3 per cent (1 in 12) change such as from 84 to 77 cannabis positive per 1,000 testees.
What Ms Eagle did not explain is why the cannabis positive rate has gone down so markedly from 2006/07 onwards. On January 18, however, she disclosed that an internal MDT audit had discovered that at a third of the establishments sampled (number sampled not specified!) there were long periods each month when no random testing was undertaken. Could this be implicated?
More strikingly, the opiate positive rate in rMDTs had been increasing from 2006/07 until curtailed by a near doubling in the prescribed methadone rate by 2008/09. Prisons’ opiate positive rate in rMDT should now be decreasing precisely due to the roll-out of methadone prescribing as part of the Integrated Drug Treatment System (IDTS), and so rMDT analyses and their reporting by Ministers need now to take this into account. See Straight Statistics in October 2009 for suggestions on how to do this.
Repeating a well-worn refrain on rMDTs does not serve prisoners’ health or the public purse on which rMDTs are an unquantified but substantial drain. Andrew Pelling MP has tried in vain to discover the actual cost.
Shailesh Vara MP was also interested in IDTS and asked: “With 20,000 prisoners on long-term methadone prescriptions and only 1,000 on an abstinence programme, have the Government got the balance right in their drugs programme in prisons?”
Ms Eagle pointed out that those who get methadone maintenance treatment in prison are those with short sentences that would not allow a proper length of time for dose reduction, and that prisons needed to offer a balance between different types and length of drug treatment.
Paul Flynn MP then related the tragic deaths of two constituents whom the Prison Service “had down as models of behaviour and success. They went in as drug users and emerged clean. Tragically, one of them lived for a week afterwards and the other for just a day. Is not the greatest danger for prisoners the point when they leave prison and go back to their old haunts?”
Straight Statistics has pointed out that in England and Wales - unlike in Scotland – there is no look-back at the prison-release history of every drugs-related death to determine how many occurred within 4 weeks of a release from prison. In Scotland, the answer is one in eight, or around 50 per year.
Better still, via prisons’ CARAT (Counselling, Assessment, Referral, Advice and Throughcare) assessments and the Integrated Drug Treatment System in England and Wales, it should be possible to record the nature of any drug treatment that the deceased had during his/her final incarceration; and similarly for, say, two randomly-sampled age/sex matched controls released from the same prison in the same fortnight as the deceased.
Indeed, I would consider that it is vital for commissioned abstinence-based programmes in prisons, and their advocates, to establish how many of their opiate-dependent former clients actually die within 2-4 weeks of release from prison.
